international – Nursing Review
https://www.nursingreview.co.nz
New Zealand's independent nursing seriesThu, 22 Feb 2018 23:41:17 +0000en-UShourly1https://wordpress.org/?v=4.9.4The non-nursing nurse’s OE
https://www.nursingreview.co.nz/the-non-nursing-nurses-oe/
https://www.nursingreview.co.nz/the-non-nursing-nurses-oe/#respondMon, 19 Feb 2018 22:11:35 +0000https://www.nursingreview.co.nz/?p=4561In April last year 25-year-old Kiwi nurse Christine Stanley headed off on her OE. After six weeks travelling through the US and Canada she arrived in the UK keen to get a job, save some money and travel through Europe.
This is a familiar path that thousands of Kiwi nurses have followed before her. In the ’50s they went by ship and in the ’70s many travelled overland via the hippy trail but the most common OE destination was the ‘mother country’, England, where New Zealand nurses could typically easily get nursing jobs, earn some money, travel and gain some experience in some of London’s top teaching hospitals at the same time.
But since 2005 registering as a nurse in the UK as a non-EU trained nurse has become increasingly more complex and expensive, resulting in Stanley being part of a new generation of Kiwi nurses on their UK OE who opt to put nursing aside for a while to work as live-in carers.
Stanley graduated in late 2014 from the University of Auckland nursing school and went to work in the surgical ward of a private hospital. With two years’ experience under her belt she decided to follow her sister and some non-nursing mates and head off.
Initially she planned to just be away for six months so didn’t think the complex and costly UK RN registration process was worth pursuing, and having heard about live-in care work she decided it sounded a much simpler option. She has now stretched her OE plans to closer to 15 months – long enough away to see a good chunk of the world but not too long from nursing to put her annual practising certificate (APC) in jeopardy.
Stanley is in the UK on a Youth Mobility Scheme (YMS) visa that allows 18–30-year-olds from New Zealand (and seven other eligible countries) to work in the UK for up to two years.
She is based in Oxford, working for agency Oxford Aunts as a level-four carer working with complex clients needing advanced-level carers. Her first client was for just a month and she has been with her second, who requires a hoist to get in and out of bed, since August.
“The downside of live-in care obviously is that you do sacrifice a bit of your social life but it is really worth it for the experience of giving one-on-one care to a person. You can really make a positive difference to their life.”
The sacrifice is rewarded by free board and food, a combination that has allowed her to save funds to travel around Europe and Asia with mates, plus have the security of slipping back into the same job on her return to UK as a reliever steps in to look after her long-term client while she takes leave.
In September she went to France, Italy and Germany for about a month; in November she spent two weeks in Europe; and she has recently returned from India and Sri Lanka and another trip to France.
Stanley says her actual hourly pay rate is similar to what she received as an RN for less stressful work, but she works more hours. Typically her contract is for 8–10 hours’ work a day – spread across the day for when her client needs her – but she has a three-hour break outside the house once a day, and once a week a reliever provides an eight-hour break, during which she can visit friends in London or head elsewhere on a day trip.
Stanley is planning to return in home in July. She says she is not tempted to stay on and seek registration, even though there appear to be nursing jobs available from what she saw online.
“The trouble is that the pay of nursing jobs is not very good in the UK – I think it’s almost worse than New Zealand from my limited research. Also if you are going to live in London to nurse, the cost of living is insane.”
For now she is planning to return to work in a surgical or medical setting to broaden her nursing skills. But she says her time as a live-in carer has made her passionate about aged care and sparked her interest in working in this area in the future. But first she has one final big trip to do before she finishes her OE and heads back downunder to resume her nursing career.
]]>https://www.nursingreview.co.nz/the-non-nursing-nurses-oe/feed/0Whangarei nurse off to help displaced Rohingya Muslims
https://www.nursingreview.co.nz/whangarei-nurse-off-to-help-displaced-rohingya-muslims/
https://www.nursingreview.co.nz/whangarei-nurse-off-to-help-displaced-rohingya-muslims/#respondWed, 08 Nov 2017 21:13:24 +0000https://www.nursingreview.co.nz/?p=3959Donna Collins’ expertise as a nurse and midwife will be tested like never before when she sets foot in makeshift border camps crowded with displaced Myanmar Muslims.
The Northland District Health Board employee from Whangarei is expected to fly out next week for Bangladesh to help hundreds of thousands of Rohingya Muslims.
Close to one million Rohingya are now living in mud huts, tents and under sheets of tarpaulin in camps outside the Bangladeshi port town of Cox’s Bazar.
In Myanmar soldiers, sometimes together with police and local Buddhists, are accused of massacres, gang-rape and arson under the guise of hunting militants, forcing the Rohingya to flee.
Red Cross opened a fully equipped field hospital in Cox’s Bazar and is providing the displaced people food, water, shelter and medical treatment.
Ms Collins will be based there from November 19 for four weeks and said the sheer scale of the humanitarian crisis has not been lost on her.
She helped during the Ebola outbreak in Africa, in the Solomon Islands last year during a dengue fever outbreak, and was part of the Red Cross disaster response team in Nepal after the 2015 earthquake.
But Bangladesh, a country she has never been to, will be her biggest challenge yet.
“The sheer number of people affected is something I’ve never seen before. It’s heartbreaking. Just the number of people arriving in camps with gunshot wounds and burns.
“Sixty per cent of those who are crossing over are women and children and that’s where my role as a nurse and midwife will be crucial.”
She said the Red Cross is doing a cholera vaccination campaign because the spread of water-borne diseases among the hungry, sick and the injured was a concern.
“My previous deployments have been as a nurse and a generalised team member but this time I’ll be providing midwifery care, which will be cool, as that’s my speciality.”
Ms Collins thanked the NDHB and her family for their support towards a worthy cause.
Red Cross estimates 604,000 Rohingya Muslims have crossed the border into Bangladesh since August 25 while hundreds more arrive every day, most of them on foot with only what they can carry. They are almost entirely dependent on humanitarian aid to survive.
In order to dramatically scale up response efforts, Red Cross urgently needs more than NZ$49 million to provide support to a further 200,000 people.
Ms Collins has urged people to donate generously so that more people can be helped.
]]>https://www.nursingreview.co.nz/whangarei-nurse-off-to-help-displaced-rohingya-muslims/feed/0‘Good as Gold’ nursing student giving back to African village
https://www.nursingreview.co.nz/good-as-gold-nursing-student-giving-back-to-african-village/
https://www.nursingreview.co.nz/good-as-gold-nursing-student-giving-back-to-african-village/#respondMon, 30 Oct 2017 22:54:21 +0000https://www.nursingreview.co.nz/?p=3819A gap year in Africa set nursing student Devon Kilkelly on a path that this month saw her win $10,000 for a village that was her home for six months and now has a place in her life for keeps.
The second year nursing student at Otago Polytechnic recently featured on Seven Sharp as the winner of an ASB Good as Gold award of $10,000 for the village preschool she has supported since first working there in 2015.
Devon says she ended up in Africa because after she left school she had no idea of what to do, apart from some vague ideas about outdoor education. So the Greymouth 18-year-old opted to take a gap year in a completely different culture with the aim of making a difference at the same time.
She ended up spending six months in 2015 as a volunteer in Ngara in Malawi – a fishing village of about 4000 people – where she taught biology and geography at the village high school, helped out at the local preschool (called Ngara Nursery) and worked at the local healthcare clinic.
The village and its ramshackle nursery captured her heart and led her to raise thousands of dollars to transform the nursery (see more below), but it was the healthcare needs of the people that captured both her head and heart and saw her choose nursing as a career on her return to New Zealand.
The village health centre had no running water and was staffed by a healthcare worker with limited training. This resulted in practices that the Kiwi school-leaver used to Western health standards knew were wrong, but had insufficient knowledge – or the standing, as a visiting teenager – to change. Practices such as poor hand sanitising, incorrect doses of medication given at the wrong intervals and treatments for a chief or a white person that differed from those given to people of lower status in the village.
Seeing what a difference nursing could make to villages like Ngara inspired Devon’s career choice.
“My dream is one day to go back over there and implement roaming nursing education – that’s where you are going to make the biggest difference,” she says. “Because there are so many small villages in Malawi, if you go to those village clinics and implement the basics like hand hygiene, standard dosages and proper disposal of infectious material…”
For example, the village clinic was delivering the birth control injection Depo Provera to village women but not emphasising how important it was to have the follow-up injection on time. “The women were given the day for the follow-up injection but the importance of having the injection on that day and not leaving it for a week or two weeks would be lost in translation.”
Or the chief would be given double the doze required of quinine, as he was an important person, in the belief that he would be cured more quickly.
The neighbouring village had a larger medical centre, staffed by local nursing students, where Devon got to help deliver 12 babies. She also got to travel to the local city to observe three surgeries, although her initial planned visit was postponed as the hospital had no power that day.
Nurses are few and far between in Malawi (World Health Organisation statistics for 2010 show that Malawi has 0.28 nurses per 1000 people, compared with New Zealand’s 10.7 per 1000 people) and Devon says the nursing students she met needed to work really hard to gain scholarships to be able to afford the three-year degree.
“It made me really want to educate myself as a nurse and continue to help people in New Zealand and also one day to be able to go back over there and share the education from my degree,” she says.
The second-year student is just finishing a paediatric placement, which she has been loving, and is keen to work in paediatrics, but with another year to go she is still open to all specialties.
Ramshackle nursery to stimulating learning environment
From her nursing studies, Devon now knows how important the first five years of a child’s life are, but as a teenager working in Ngara Nursery school, it was all too clear that urgent work was needed.
The nursery works as both a crèche and a pre-school for the village, where many women start work early in the morning in the maize fields to avoid the heat or make products to sell in roadside markets.
When Devon and her English fundraising partner Daisy first started working at the village nursery in 2015, it had large holes in the concrete floor, paint coming off the walls and a long-drop toilet without a door.
The children arrived hungry – poor village families usually skip breakfast and prioritise a large lunch and dinner. There were only five toys to share between 20 children, the teacher had no blackboards and no training, and the children had nothing to write or draw on. “It was very unstimulating and very dangerous actually,” says Devon.
By the time Devon left, thanks to fundraising support from her and Daisy’s home town, the floor was fixed, the toilet had a door, there were wall-hung blackboards for the teacher, slates for the children, new toys and sports equipment and a safe water supply. The teacher was being funded to undertake some early childhood training and the children were having porridge for breakfast. “Now our roll has grown to 90 children – it is so big we are having to split into two different age groups.”
Devon says the nursery school is also very important to help prepare children for primary school, particularly as in Malawi the children in primary school are taught English right from the start. “But obviously their families speak to them in the local language, so a lot of the time the children don’t know any English and aren’t exposed to it until they start primary school. So they are lost and the school class sizes can be 80 to 100 students per teacher.
The nursery school provides the chance to give them a great ‘kick start’ before primary school and Devon says from her nursing studies she also now knows how important developmentally it is to stimulate children’s brains from a young age.
Since Devon’s return to New Zealand her support of Ngara nursery has continued – her commitment is one she hopes to continue for the rest of her life. “To feed a child a bowl of porridge is 8c a bowl and for 90 children five days a week that is $7.20 for a day – not much more than a takeaway coffee – or $36 for the week,” says Devon. “When you put it like that and then you think how many of us buy at least one takeaway coffee a week…”
Devon has sold electronic fly swats to raise funds; last year she ran the Dunedin half-marathon and this year she began reaching out to her new community of Dunedin to raise funds for further nursery goals, including continuing to provide the children with porridge and a teacher, a new building, more toys and learning materials, and a playground.
Thanks to Devon’s ASB Good as Gold win, some of those goals will now be met, with her plan being to use some of the money to renovate a community building 30 metres down the road as an extension of the nursery school. “It is just awesome that we are able to grow and house this expansion.”
She is also buzzing that the recent television coverage of her fundraising work for the nursery saw an Auckland playground company, Parks Supplies, offer to donate a playground for the nursery’s children.
“Now I’m in the midst of figuring out how to get it over to Malawi,” says an excited Devon. This is no easy task, but, based on her work to date, is certainly not beyond this 20-year-old ‘good as gold’ nursing student.
You can find out more about Devon’s project on her Givealittle page.
]]>https://www.nursingreview.co.nz/good-as-gold-nursing-student-giving-back-to-african-village/feed/0Cook Islands nurse appointed WHO Chief Nurse
https://www.nursingreview.co.nz/cook-islands-nurse-appointed-who-chief-nurse/
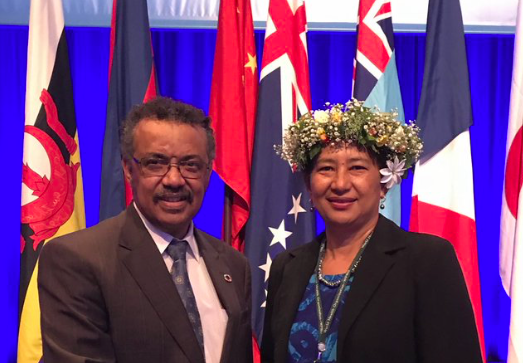
https://www.nursingreview.co.nz/cook-islands-nurse-appointed-who-chief-nurse/#respondFri, 13 Oct 2017 05:25:11 +0000https://www.nursingreview.co.nz/?p=3580Another nurse with New Zealand connections has been appointed to a world-leading role with the announcement that Cook Islands nurse Elizabeth Iro is WHO’s new Chief Nurse.
Iro, who has been a nurse and midwife in New Zealand, is currently the Cook Islands Secretary of Health and is the former Cook Islands Chief Nursing Officer and a former president of the Cook Islands Nurses Association.
WHO Director-General Dr Tedros with new WHO Chief Nurse Elizabeth Iro.
Her appointment was announced this week in Brisbane by Dr Tedros Adhanom Ghebreyesus, WHO Director-General. It follows Dr Tedros pledging in May this year at the International Council of Nurses (ICN) Congress in Barcelona that he would reinstate a nursing role in his WHO headquarters team in Geneva.
Until recently also based in Geneva was former New Zealand chief nurse Dr Frances Hughes, who was chief executive of ICN from early 2016 until August this year. Also in Europe is New Zealand midwife Dr Sally Pairman who in January this year was appointed the chief executive of the International Confederation of Midwives.
On accepting the position, Iro said she was very honoured and humbled by the announcement.
“I think this appointment is going to be raising the profile of nursing and midwifery and I anticipate it will be encouraging and enabling for nurse to work to their full potential if countries are to achieve universal health coverage.”
Elizabeth Iro, WHO Chief Nurse.
Iro has more than 30 years’ experience in public health in the Cook Islands and New Zealand. For the first 25 years of her career she was a staff nurse, midwife and charge midwife at hospitals in the Cook Islands and New Zealand.
As president of the Cook Island Nurses Association in 2005, she helped to negotiate a salary increase for the country’s then-78 nurses after the nurses threatened a nationwide strike.
The nurse leader, who has master’s degrees in business administration and health science, went on to become the Chief Nursing Officer. In 2012 she became the first nurse to head the Cook Islands Ministry of Health when she became Secretary of Health.
As Secretary of Health she has implemented health reforms, including developing the country’s National Health Roadmap 2017-2036, the National Health Strategic Plan 2017-2021, and the Health Clinical Workforce Plan. In addition, she has helped to develop the Cook Islands Fellowship in General Practice, a postgraduate training fellowship for doctors working in the Cook Islands.
ICN president Annette Kennedy said ICN was “delighted” that Dr Tedros was true to his word and had reinstated the chief nurse role at WHO (after a seven-year gap). “ICN has met with Dr Tedros several times in the past few months to lobby for this position. He clearly recognises the value of nurses and has followed through on his promises.”
“I am thrilled to welcome Ms Iro to our team as WHO’s Chief Nursing Officer,” said Dr Tedros. “Nurses play a critical role not only in delivering healthcare to millions around the world, but also in transforming health policies, promoting health in communities, and supporting patients and families. Nurses are central to achieving universal health coverage and the Sustainable Development Goals. Ms Iro will keep that perspective front and centre at WHO.”
Kennedy said that ICN would continue to work closely with WHO to ensure that nurses had a chair at the policy-making table. “ICN looks forward to working closely with the WHO Chief Nurse and Director-General to support their work and represent the global nursing voice,” she said.
Iro’s appointment is the latest addition to the senior leadership team Dr Tedros announced last week, which includes representatives from every WHO region and is 60% women. It came at the 68th session of the WHO Regional Committee for the Western Pacific, which took place from 9 to 13 October 2017 in Brisbane.
Elizabeth Iro is married with three children.
*The article was revised on October 10 2017.
]]>https://www.nursingreview.co.nz/cook-islands-nurse-appointed-who-chief-nurse/feed/0How health workers can spot and help “modern slaves”
https://www.nursingreview.co.nz/how-health-workers-can-spot-and-help-modern-slaves/
https://www.nursingreview.co.nz/how-health-workers-can-spot-and-help-modern-slaves/#respondThu, 05 Oct 2017 20:42:39 +0000https://www.nursingreview.co.nz/?p=3504Frontline health workers can help victims of “modern slavery”, researchers say.
While many of us might think of slavery as a tragedy of a bygone area, a group of experts writing in the New Zealand Medical Journal today say a hidden modern slavery problem persists today.
This includes forced, underage and servile forms of marriage, and worker exploitation.
The International Labour Organisation estimates there are nearly 21 million victims of slavery worldwide, and while there were no specific figures for New Zealand, our country was first described by a 2004 US report as a destination country for people trafficked for sexual exploitation.
The new paper’s authors highlight many other examples, including migrant fishers and horticulture workers promised well-paying jobs and work permits – with one Fijian earning as little as $25 for three weeks’ work.
Now, they say, our doctors and health workers are in a unique position to help and advocate for them.
“Slavery has serious health consequences, but is a mostly neglected issue within the health system,” said lead author Dr Paula King, a public health physician and Otago University clinical research fellow.
“Victims are at increased risk of acute and chronic physical and mental health problems, injuries from dangerous living or working conditions, or physical or sexual abuse, so they are likely to come into contact with health workers.
“We know that health workers may have had contact with people in situations of slavery, but may not have had the knowledge, resources or skills to identify victims and offer effective help.”
Examples of scenarios that should ring alarm bells for health workers include migrant workers with “workplace injuries” accompanied by a “superior” who insists on rushing treatment to get them back to work.
Another case might be an infectious outbreak where it was found workers were living together in crowded conditions.
Victims may go to the doctor for routine care, but show telltale signs of exploitation such as unexplained injuries, contradictions in their stories and behaviour, not knowing their home address or lack of personal identification.
Co-author Dr Christina Stringer of the University of Auckland’s Business School published a report last year revealing the exploitation of migrant and New Zealand-born workers across many industries, including horticulture, hospitality and construction.
“One migrant we interviewed was beaten up in an orchard by his contractor, while another was physically assaulted and denied sufficient food; he ran away and was found sleeping on the streets in a distressed state,” Stringer said.
“There is also evidence of exploitation in the health and aged-care sectors themselves.”
More than 70 businesses were banned from hiring migrant workers for breaching labour laws in the last six months.
“Slavery is a violation of many human rights, including the right to health,” King said.
“Doctors and other health workers hold a privileged position in the health sector and can, and should be, leading advocates for change at government, health system and organisational levels to address slavery and its health consequences.
“A robust health response to slavery includes the ability to identify current victims or those at risk, and to treat them in a culturally competent and trauma-informed manner in collaboration with other services.”
Health workers could assist by making themselves more aware of the problem, linking up with groups working with migrants and refugees, and taking the lead in developing new guidelines and policy within their organisations and professional bodies.
]]>https://www.nursingreview.co.nz/how-health-workers-can-spot-and-help-modern-slaves/feed/0Fighting falls not fires: UK firefighters take role in falls prevention
https://www.nursingreview.co.nz/fighting-falls-not-fires-uk-firefighters-take-role-in-falls-prevention/
https://www.nursingreview.co.nz/fighting-falls-not-fires-uk-firefighters-take-role-in-falls-prevention/#respondWed, 27 Sep 2017 17:51:23 +0000https://www.nursingreview.co.nz/?p=3351Fall prevention specialists from the UK, Australia and New Zealand came together earlier this month to discuss and share approaches to reducing harm from falls in Health Quality & Safety Commission forums in Auckland and Wellington.
Dr Frances Healey, a nurse and deputy director of Patient Safety for the National Health Service (England), said the three nations faced similar challenges and had similar programmes but were all in slightly different places on the journey. She said what many of the forum conversations centred on were the “smaller, human aspects” of falls prevention work, like a recent initiative in the UK using firefighters to deliver exercise programmes for the elderly at the local fire station.
“It is much more attractive to elderly men because it was very manly,” said Healey.
Julie Windsor, the patient safety clinical lead for older people for NHS (England), told Nursing Review that the firefighter initiative grew out of firefighters being so successful in raising fire awareness and fire safety that they had “almost done themselves out of a job”.
She said the chief fire officers realised they had a highly skilled workforce that was possibly being underutilised. Firefighters were also highly trusted and had no particular stigma attached to them as a fire could happen to anybody.
In 2015 firefighters joined forces with the NHS, Age UK, Public Health England and the Local Government Association to sign a new health partnership to help tackle health and social problems, including turning fire service ‘Home Safety’ checks into ‘Safe and Well’ visits to help the vulnerable and those with complex conditions in particular. The aim was not only to reduce the risks of a fire but also to look at reducing falls, loneliness and isolation by spotting hazards like loose rugs, and to signpost people – from the elderly to young families – to local groups for help, support or company.
Windsor said what grew out of this partnership was a further initiative for firefighters to offer exercise programmes for the elderly to help reduce their chances of falling.
She said firefighters were required to be physically fit, “so they looked the part”, and they already had spaces at their stations with exercise equipment. Existing falls prevention services stepped in and trained the firefighters in the correct, evidence-based exercise programme, which the firefighters deliver at the neighbourhood firestation to the elderly in the area.
“The older men, and some of the older woman I must say, have found it a very attractive proposition to go along to the local firestation to be trained by the fire crew,” said Windsor. She said they are run as adjuncts to existing community balance and safety classes but the firefighter classes seemed to be a popular alternative – particularly for the men who might prefer not to go to community classes that are often mostly women.
(Recently New Zealand launched the Live Stronger for Longer website to promote approved community exercise classes for the over-65s to help build leg and core strength to improve balance and reduce the risk of falls. More information at live stronger.org.nz.)
New Zealands’ positive imagery and Oz’s sensitive questions
Healey believes the real value of the tri-nations forum was not in sharing the high-end level areas – such as educational programmes and service provision, where the three countries were already going in the same direction – but in the “little human differences” that fascinate people. So major projects, such as the UK’s now well-established national hip fracture database that had been a “very powerful force” for improvements in service provision and service delivery for older people, had not been discussed at great length.
But what had captured many at the tri-nations forum had been initiatives such as the UK firefighters. Another was an approach to reducing falls by dementia patients in hospital – shared by Lorraine Lovitt, the lead for the New South Wales falls prevention programme – which involved nurses asking the patient’s families what the five most important things were for them to know about their loved one.
Healey said as a visitor from the UK something that particularly struck her was how “positive, cool, fun and even trendy” the images were of older people in the New Zealand falls awareness material. “And that positive imagery is so important to have, rather than the person with the Zimmer frame.”
She said the UK had a variation on this with its ‘Don’t mention the F-word’ campaign, which was where older people used “some fairly colourful analogies” about not wanting to be associated with ‘falls’ and ‘frailty’.
]]>https://www.nursingreview.co.nz/fighting-falls-not-fires-uk-firefighters-take-role-in-falls-prevention/feed/0‘One tough cookie’: defence nursing from Somalia to Afghanistan
https://www.nursingreview.co.nz/one-tough-cookie-defence-nursing-in-somalia-to-afghanistan/
https://www.nursingreview.co.nz/one-tough-cookie-defence-nursing-in-somalia-to-afghanistan/#respondMon, 18 Sep 2017 18:05:46 +0000https://www.nursingreview.co.nz/?p=3164Not many nurses have wielded an assault rifle to defend their patient in the Somalian desert. The Bay of Plenty Times profiles retired army nurse Judith Telford.
Judith Telford cocked her Steyr semi-automatic assault rifle.
It was the summer of 1994 and there was no time to think about who might fire first. Her Saint Christopher pendant clung to perspiring skin. She lifted her firing arm higher, the red cross emblem on her upper limb clearly visible.
This wasn’t how she’d imagined nursing: stuck in this God-forsaken place in the Somali desert, risking her life for another.
She and her flight nurse colleague stood on each side of their Bell212 Canadian helicopter. Inside an injured Somali wriggled. “You’ve got our brutha,” the approaching group of Somalis spat.
Alone in the desert, Telford’s military team had lost their number one engine on takeoff. They returned to this spot, an airstrip popular for drug runs. Alone with no radio, while the pilots and doctor returned to their compound to request a replacement chopper, the two women clung to their weapons.
“You’ve got our brutha,” the ascending group repeated. “Back off,” Telford said, cocking her rifle. And they did.
Measuring a mere 1.549 metres, Telford is one tough cookie.
Nurse Judith Telford protects injured patient.
The 57-year-old Papamoa woman disagrees her career is anything extraordinary, but her war stories tell you otherwise.
She was “married” to the military for 28 years and posted 15 times with the Royal New Zealand Nursing Corp and Air Force, with three major deployments to Somalia, Afghanistan and East Timor.
Most memorable was the ’94 Somalia trip. The Kiwi contingent arrived in the Horn of Africa not long after two American Black Hawk helicopters were shot down. She was the only medic in the 65-plus contingent, and for seven months found herself challenged, stressed and frightened like she’d never been before. “It was the pits, really.”
The military had their own compound that Somalis would work in during the day. At around 2pm, the Somalis would knock off and chew the drug khat, a flowering plant.
“The next thing, you’d have scuds (missiles) coming over you. They’d be having warlord fights. When you went out of the compound, you were always in a convoy, always armed. Weapons out the window … Because it was so unpredictable.” Even children couldn’t be trusted.
Carrying a semi-automatic weapon was standard kit for Telford, who was right-sighted but left-handed. Normally officers carry pistols but the military didn’t have enough to go around.
She recalls landing in a grid reference and she and her team had no idea how they were going to be received. “A couple of times we were literally running out of the village with a casualty. We would check our aircraft every day we landed and see how many holes had gone through.”
To add to this insanity, Somali women in burkas, some pregnant, were placed in front of armed men as shields. “Women and children were worthless to the Somalis. Camels were far more important.”
The experience changed her outlook on life, and she grew up quickly.
Stuck in the Kiwi contingent compound, Taniwha Hill, missiles would fly overhead and bullets whizzed through their tent line.
Injury-wise, she treated everything from gunshot wounds to malaria, dengue fever, Aids and shark bites. There were maimed children, and children who had been burnt by their parents to rid them of “the evil spirit”.
A women’s clinic was set up to provide contraceptives, but it was a fruitless exercise.
“You couldn’t give them a packet of pills because they would sell that. So, they would come in each day for their tablet, and come back pregnant.”
The women would hide the pill in a hole in their teeth and gave it to the chickens because the hormones made chickens fat. “It’s a backwards country but very innovative, you know?”
Sharing these stories, there’s nothing visible to indicate Telford was once a woman dressed for conflict.
Today, she has a rainbow-coloured crystal stud in each ear, shaped like a tiny dress. Her lips are painted coral, the same colour as her shirt.
On retirement from the military, she had to hand her uniforms back, but still has her heavy black boots and green flight suit.
She has a room in her house adorned with photos, certificates, badges, berets and her lemon squeezer. As a side note, she got the lemon squeezer stuck in a rolled up tent line when meeting patron for the Royal New Zealand Nursing Corp, Princess Anne.
Pride of place in her lounge is a skinny panoramic photograph of Somalia. She’s seen more gore and heartache than most hardened medical professionals in New Zealand.
Judith Telford in Afghanistan, Bahmian province on a reconnaissance mission.
Telford began her career at Waiouru Military Camp in 1985 and rose through the ranks from lieutenant to squadron leader.
She’s worked in neurosurgery, as a trauma nurse, Defence Health Services school instructor and a flight nurse bringing sick and injured Kiwis back home from as far away as New York.
“Nursing in an aircraft, it’s my passion.”
She was initially scared about hanging up her military uniform.
“You live in this big family for 28 years and it’s kind of like there’s civvy street, and us. Going back out, I just didn’t know how well I would cope.
“People say to me: ‘Did you get married? And I say: I married the military. Like, I have had a number of boyfriends, but it was all about my career.”
And of children: “I guess you just get to the age where you go, ‘I would be really selfish if I had a child now.’ … It had to be the right circumstances, and that didn’t happen. I enjoy my nieces and nephews.”
The youngest of three children and the only girl, she’s at a point in her life where she can afford to be open.
“Knowing that I don’t have to deploy again, I can be a lot more honest. Sometimes the worst thing you’re seeing isn’t the gore and the detail. It’s the total destruction … Why are we here? Why are we doing this?”
In 2002 she helped in the transportation of patients from the Bali bombings, travelling in a Hercules with an air force sergeant and three civilians.
“We were meant to bring back three people … Two never made it, they died on route, and the third person, Darcia, was burnt from head to foot.
Did she ever get used to seeing tragedy? She says “yes”.
“There’s something about putting on a uniform. It kind of protects you. You just get in there and do your job. And then afterwards, you think about it.”
She has countless photos from her deployments. One shows her resuscitating a baby in the troops’ deployable hospital in East Timor in 2000. The baby, a twin, had been brought in by helicopter from a remote area.
“You know, you have to say to yourself, if they can’t breathe on their own, what are we doing? Because you can’t incubate them. There is no paediatric intensive care in East Timor.”
She tells another story of a 16-year-old girl suffering a pulmonary embolism and dying in a medical tent of respiratory distress. Medics transported her body back to her remote village.
“The whole village came out and [we] just got swamped. We got quite a bad name. ‘Don’t go to the white man’s hospital because you come out dead,’ and that wasn’t untrue because we would see the worst cases. They’d already been to their medicine man, and came to us as their last ditch.”
Staff were required to go through a post deployment brief on the way home. Humour got them through a lot, she says.
She was with the NZ Nursing Corps tri-service corps for 20 years, before going full-time with the Air Force in 2005 when she took on the task of setting up a new state-of-the-art “aero-medical capability” (aka a flying hospital) in a Boeing 757.
She resigned when the project stagnated. “I completed as much as I could do and we were waiting for certification which is an extremely long, drawn-out process. Military was going down a different line; it had a new generation shaping it [and it] was time to move on.”
Her exit included one last mission to the US. Telford joined the team who flew on a Boeing to Washington DC to bring injured soldiers who’d been fighting in Afghanistan home. It was a 2.5 day journey.
“I couldn’t have been prouder … It makes me feel emotional just thinking about it. It was such a perfect way to end my military career to see this capability finally used.
“[Working at altitude] is not like an ED department. You can’t go ‘crash team’: there is no crash team, you’re it. Once you’re in the air, you’re in the air. It’s a challenging, challenging environment.”
Following her retirement from the Defence Force at the end of 2013, she worked in aged care in Hamilton and Cambridge. A move to Papamoa with Burmese cats Louie and Lacey and Cairn Terrier Chardonnay, beckoned last year. After a stint as hospital coordinator at Cedar Manor, she secured her “dream job” as a community advisor at the Stroke Foundation.
These days she lives a much quieter life of cross-stitch, cooking and gardening. Few, if any, of her clients know of her background. Some don’t even know she’s a nurse. She speaks at women’s clubs but doesn’t see herself as “anyone special”.
“There will always be wars,” she muses. “The war today is just unpredictable, happens anytime, anyplace. You just see it every night on the news, don’t you? Another suicide bomber. How do you fight against that? People don’t do a 20-year [military] career any more. It’s five years … Young people get it there, grow up, get challenged, might do a tour, come back, get out.”
The other day, a Hercules roared over Tauranga. As Telford searched the sky, a kaleidoscope of memories hit her.
One day she’ll write a book. The only problem: “Where do you start? Where do you finish?”
]]>https://www.nursingreview.co.nz/one-tough-cookie-defence-nursing-in-somalia-to-afghanistan/feed/0US nurse’s violent arrest puts patient-consent law in spotlight
https://www.nursingreview.co.nz/us-nurses-violent-arrest-puts-patient-consent-law-in-spotlight/
https://www.nursingreview.co.nz/us-nurses-violent-arrest-puts-patient-consent-law-in-spotlight/#respondMon, 04 Sep 2017 09:28:11 +0000https://www.nursingreview.co.nz/?p=2797American nursing organisations and others have spoken out about the violent arrest of a Utah nurse for taking an ethical stand on patient consent, reports the Washington Post.
The videotaped arrest of a nurse at a Salt Lake City hospital – after she told police, correctly, that they weren’t allowed to draw blood from an unconscious patient – has been roundly condemned by national nursing organisations, Utah officials and even the local police department.
The July 26 incident, captured by an officer’s body camera, was made public last week after the nurse came forward. Since then, several groups have echoed the nurse’s outrage, calling for greater consequences for the police detective in question and demanding increased awareness of patient-consent laws.
In the footage, Jeff Payne, a detective with the Salt Lake City Police Department, confronts Alex Wubbels, a nurse in the burn unit at the University of Utah Hospital, over her polite but firm insistence that police could not collect blood samples from a badly injured patient. Payne didn’t have a warrant, Wubbels pointed out. And the patient wasn’t conscious, so he couldn’t give consent.
Wubbels cited hospital policy in the video – showing Payne a printout of the rules just before he abruptly arrests her – but her actions also were in line with a decision by the US Supreme Court, which explicitly ruled last year that blood can be drawn from drivers only for probable cause, with a warrant.
In the moment, none of that seemed to matter to Payne, who snapped, seized hold of Wubbels, shoved her out of the building and cuffed her hands behind her back. A bewildered Wubbels screamed “help me” and “you’re assaulting me” as the detective forced her into an unmarked car and accused her of interfering with an investigation.
Wubbels, who was not criminally charged, played the footage at a news conference last Friday with her lawyer. They called on police to rethink their treatment of hospital workers and said they had not ruled out legal action.
“I just feel betrayed, I feel angry, I feel a lot of things,” Wubbels said then. “And I’m still confused.”
Judging by the overwhelming reaction to the video, which has since been widely shared, many agree with Wubbels.
The department said two of its employees had been placed on administrative leave, pending the results of an investigation, but did not give details. A criminal investigation is underway, according to Salt Lake County District Attorney Sam Gill, and the city’s mayor and police chief apologised to Wubbels in a statement.
“What I saw is completely unacceptable to the values of my administration and of the values of the Salt Lake City Police Department,” Mayor Jackie Biskupski said. “I extend a personal apology to Ms Wubbles for what she has been through for simply doing her job.”
However, the Salt Lake Tribune editorial board called for harsher consequences, saying the incident had raised “serious questions” about the city’s police department and wondering why Payne had not been fired immediately.
“Unless the investigations turn up something that is not now apparent, it seems clear that Payne should already have lost his job, and that his certification to be a law enforcement officer should be permanently revoked,” the board wrote.
“The fact that he was removed from the roll of officers who are allowed to take blood samples, but not placed on leave until the matter became public and a criminal investigation launched, can only serve to undermine public confidence in the whole department.”
The Utah Nurses Association stated it was “deeply disturbed” by the video, and encouraged as many people as possible to view it to understand a nurse’s “ethical duty to act in the best interest of our patients at all times and in all settings”.
Nurses are bound by a code of ethics that dictates they must first promote the rights, health and safety of the patient, according to the American Nurses Association. By all measures, Wubbels followed that code.
“It is outrageous and unacceptable that a nurse should be treated in this way for following her professional duty to advocate on behalf of the patient as well as following the policies of her employer and the law,” ANA President Pam Cipriano said. “Nurse Wubbels did everything right. It is imperative that law enforcement and nursing professionals respect each other and resolve conflicts through dialogue and due process.”
Even if Payne believed he had “implied consent” to draw the patient’s blood, it would not have applied under these circumstances, since Payne was trying to prove that the driver was not under the influence, criminal law professor Paul Cassell wrote in a guest piece for the Salt Lake Tribune.
“The ultimate requirement of our Constitution is that police must behave reasonably,” Cassell wrote for the newspaper. “Handcuffing a nurse and throwing her into a squad car is, given all of the circumstances here, not reasonable – and, it turns out, was not ultimately supportable under Utah law.”
The encounter started on July 26 when a suspect speeding away from police in a pickup truck on a Utah highway smashed head-on into a truck driver, as local media reported. Medics sedated the truck driver, who was severely burned, and took him to the University of Utah Hospital. He arrived in a comatose state, according to the Desert News. The suspect died in the crash.
A neighbouring police department sent Payne, a trained police phlebotomist, to collect blood from the patient and check for illicit substances, as the Tribune reported. The goal was reportedly to protect the trucker, who was not suspected of a crime. Payne’s lieutenant ordered him to arrest Wubbels if she refused to let him draw a sample, according to the Tribune.
Since the footage was made public, the unconscious patient has been identified as William Gray, a reserve officer with the Rigby Police Department in Idaho, who is a full-time truck driver. That department said in a statement that it had not been aware of the incident until video of Wubbels’s arrest went viral, and it praised the nurse for her actions.
]]>https://www.nursingreview.co.nz/us-nurses-violent-arrest-puts-patient-consent-law-in-spotlight/feed/0Free e-learning module for health professionals on working with interpreters
https://www.nursingreview.co.nz/free-e-learning-module-for-health-professionals-on-working-with-interpreters/
https://www.nursingreview.co.nz/free-e-learning-module-for-health-professionals-on-working-with-interpreters/#respondWed, 30 Aug 2017 04:22:39 +0000https://www.nursingreview.co.nz/?p=2743Video clips of nurses working with interpreters are part of a new e-learning module aimed at helping clinicians be more confident with including interpreters in patient consultations.
The module has been developed by a team of researchers at the University of Otago, Wellington, to provide ‘realistic and practical guidance’ for nurses and doctors working with interpreters, particularly in primary health care. It was a response to the growing number of new New Zealanders – both migrants and refugees – with limited proficiency in English and builds on research carried out since 2009 into using interpreters in primary care.
One of the module developers, Jo Hilder, said professional interpreting services were increasingly available but were still under-utilised and it was hoped the learning module would help both practising clinicians and students to be more aware and confident of working with interpreters.
The module features a toolkit of flowcharts and tables that highlight what to consider when making decisions on the best approach for a given situation and the pros and cons of the different interpreting options, including using family. Hilder said they used authentic video footage, with the full consent of all involved, of real doctors and nurses working with patients and interpreters.
The learning package covers a range of topics, including practice advice on seating arrangements and the extra care and skill required if nurses and doctors are considering using patients’ family members as an interpreter option. The focus of the module is on spoken language, but it also provides some information on interpreting NZ Sign Language for deaf patients. The authors also point out that the module is focused on primary health care and there would be slightly different needs for other forms of care, such as mental health care, in-patient care and emergency department care.
]]>https://www.nursingreview.co.nz/free-e-learning-module-for-health-professionals-on-working-with-interpreters/feed/0Research: missed nursing cares due to low staffing increases patient mortality
https://www.nursingreview.co.nz/research-missed-nursing-cares-due-to-low-staffing-increases-patient-mortality/
https://www.nursingreview.co.nz/research-missed-nursing-cares-due-to-low-staffing-increases-patient-mortality/#respondFri, 25 Aug 2017 00:29:56 +0000https://www.nursingreview.co.nz/?p=2685Missed cares are the missing link in understanding why hospitals with lower registered nurse (RN) staff levels have a higher risk of death, say the researchers whose study was published online this week in the International Journal of Nursing Studies.
The findings are the latest analysis from the RN4CAST study that connected nursing levels, the outcomes of more than 400,000 patients and survey data from 25,000 nurses working across 300 hospitals in nine European countries (including England, the Netherlands and Ireland). The latest research was lead by Dr Jane Ball of the University of Southampton and fellow authors included co-director of the RN4CAST study, Professor Linda Aiken of the University of Pennsylvania.
Ball said for years it was known there was a relationship between nurse staffing levels and hospital variation in mortality rates, but there had not been a good explanation as to how or why. However, links had now been found between lower RN staffing levels, missed patient cares and increased risks of patient death. Each 10 per cent increase in cares left undone was associated with a 16 per cent increase in the likelihood of a patient dying.
The study analysed nurses’ responses to the survey question: “On your most recent shift, which of the following activities were necessary but left undone because you lacked the time to complete them?” and presented nurses with a list of 13 activities (see list below).
The nurses surveyed were also asked how many staff were providing direct care on their last shift and how many patients were on the ward at the time.
Previous analysis of the survey showed that lower nurse staffing levels are associated with higher mortality, but Ball said the further analysis gave the “clearest indication yet that RN staffing levels were not just associated with patient mortality, but that the relationship may be causal”.
“If there are not enough registered nurses on hospital wards, necessary care is left undone and people’s lives are put at risk,” added Dr Ball.
Co-author Luk Bruyneel from KU Leuven in Belgium said the findings had implications for healthcare managers and policymakers. “Monitoring missed care may offer a more responsive and sensitive early-warning system for hospitals to detect problems before patients die,” he said. “More work needs to be done worldwide to ensure we utilise this data for the benefit of patients.”
The analysis also looked at nurses’ qualifications and confirmed that hospitals with higher numbers of registered nurses trained at degree level had a lower risk of patient mortality.
Professor Peter Griffiths, Chair of Health Services Research at the University of Southampton, said the study reinforced the importance of RNs who were trained to degree level. “It is more evidence that shows that you cannot substitute fully qualified RNs with less qualified staff without taking a risk with patient safety,” said Griffiths. “It is the number of RNs on duty that is key to ensuring complete care and minimising the risk of patients dying.”
Article reference:
Jane Ball, Luk Bruynell, Linda H. Aiken et al (2017). Post-operative mortality, missed care and nurse staffing in nine countries: A cross-sectional study. International Journal of Nursing Studies (published online open access)
The patient cares asked about in the RN4CAST nursing survey were:
adequate patient surveillance
skin care
oral hygiene
pain management
treatments and procedures
administering medication on time
frequently changing the patient’s position
comforting/talking with patients
educating patients and family
preparing patients and families for discharge
developing or updating nursing care plans/care pathways
 Red Cross opened a fully equipped field hospital in Cox’s Bazar and is providing the displaced people food, water, shelter and medical treatment.
Red Cross opened a fully equipped field hospital in Cox’s Bazar and is providing the displaced people food, water, shelter and medical treatment.

 The neighbouring village had a larger medical centre, staffed by local nursing students, where Devon got to help deliver 12 babies. She also got to travel to the local city to observe three surgeries, although her initial planned visit was postponed as the hospital had no power that day.
The neighbouring village had a larger medical centre, staffed by local nursing students, where Devon got to help deliver 12 babies. She also got to travel to the local city to observe three surgeries, although her initial planned visit was postponed as the hospital had no power that day. By the time Devon left, thanks to fundraising support from her and Daisy’s home town, the floor was fixed, the toilet had a door, there were wall-hung blackboards for the teacher, slates for the children, new toys and sports equipment and a safe water supply. The teacher was being funded to undertake some early childhood training and the children were having porridge for breakfast. “Now our roll has grown to 90 children – it is so big we are having to split into two different age groups.”
By the time Devon left, thanks to fundraising support from her and Daisy’s home town, the floor was fixed, the toilet had a door, there were wall-hung blackboards for the teacher, slates for the children, new toys and sports equipment and a safe water supply. The teacher was being funded to undertake some early childhood training and the children were having porridge for breakfast. “Now our roll has grown to 90 children – it is so big we are having to split into two different age groups.”